Target lipid fractions in secondary cardiovascular prevention
DOI:
https://doi.org/10.35954/SM2016.35.2.2Keywords:
Cardiovascular disease, Secondary Prevention, Lipoproteins, Hidroxymethylglutaryl-CoA Reductase Inhibitors.Abstract
Introduction
Cardiovascular disease is the leading cause of mortality in Uruguay and in the world. The management of lipid The management of lipid fractions is key to reduce the risk of new cardiovascular events in patients in secondary cardiovascular prevention.
In this study we analyze the proportion of patients reaching lipid goals and the presence of Residual Lipid Risk, as well as more variables with which it is associated.
Methods
We analyzed the electronic records of all the patients attended at the Secondary Cardiovascular Prevention Unit in the Cardiovascular Secondary Prevention Unit in the period from March 2014 to March 2015.
Results
A total of 287 patients were included in the study, 19.4% non smokers, 29.4% diabetic, 99.7% overweight-obese.
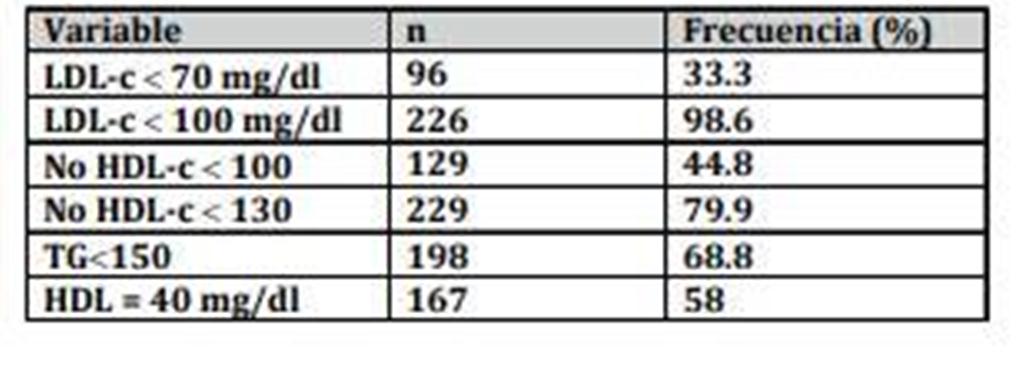
The proportion of patients with target LDL-c less than 70 and non-HDL-c less than 100 was 33.3% and 44.8% respectively.
High-dose statins were indicated in 83.1% of patients.
In those who received high doses of statins, the LDL-c goal was higher than in the group treated with moderate or low doses, 33.9% of the patients.
moderate or low doses, 33.9% vs 33.9% (p= 0.006). A Lipid Risk was Residual Lipid Risk was found to be 49.7%. The RLR was higher in diabetics, 60.2% vs 46.5% (p=0.035), in overweight-obese 88.8% vs. 70.4% (p=0.000) and in smokers or former smokers or former smokers 86.0% vs. 14.0% (p=0.023).
Conclusions
High doses of statins were associated with meeting LDL-c goals. However, it is still necessary to maximize intervention measures to achieve these goals in higher proportions.
The prevalence of Residual Lipid Risk was high, and was statistically associated with diabetes, overweight-obesity and smoking, ex-smoking. A more detailed analysis of the causes of not receiving high-dose statins associated or not with Ezetimibe and a comprehensive approach to risk factors, especially smoking and overweight-obesity, is imperative to improve the target ratio of lipid fractions in order to reduce cardiovascular risk in this group of patients.
Downloads
References
(1) Piepoli M, Hoes A, Agewall S, Albus C, Brotons C, Catapano A, et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice. Eur Heart J 2016; 37(29):2315-81.
(2) Mihaylova B, Emberson J, Blackwell L, Keech A, Simes J, Barnes E, et al. The effects of lowering LDL cholesterol with statin therapy in people at low risk of vascular disease: meta-analysis of individual data from 27 randomised trials. Lancet 2012; 380(9841):581-90.
(3) Jacobson T, Ito M, Maki K, Orringer C, Bays H, Jones P, et al. National Lipid Association recommendations for patient-centered management of dyslipidemia: Part 1–executive summary. J Clin Lipidol 2014; 8(5):473-88.
(4) Stone N, Robinson J, Lichtenstein A, Bairey Merz C, Blum C, Eckel R, et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2014; 63(25 Pt B):2889-934.
(5) Lloyd-Jones D, Morris P, Ballantyne C, Birtcher K, Daly D, et al. 2016 ACC Expert Consensus Decision Pathway on the Role of Non-Statin Therapies for LDLCholesterol Lowering in the Management of Atherosclerotic Cardiovascular Disease Risk. J Am Coll Cardiol 2016; 68(1):92-125.
(6) Núñez-Cortés J, Montoya J, Sala X. Riesgo residual vascular de origen lipídico. Estrategias para el tratamiento del riesgo residual por dislipidemia aterogénica. Clin Invest Arterioscl 2011; 23(5):230-9.
(7) Gaede P, Lund-Andersen H, Parving H, Pedersen O. Effect of a multifactorial intervention on mortality in type 2 diabetes. N Engl J Med 2008; 358(6):580-591.
Published
How to Cite
Issue
Section
License
Until 2024 we use the Creative Commons Attribution/NonCommercial Attribution 4.0 International License https://creativecommons.org/licenses/by-nc/4.0/deed.es. Which states that: you are free to share, copy and redistribute the material in any medium or format, as well as to adapt, remix, transform and build upon the material. Under the following terms:
Attribution: you must give proper credit , provide a link to the license, and indicate if changes have been made . You may do so in any reasonable manner, but not in such a way as to suggest that you or your use is endorsed by the licensor.
NonCommercial: you may not use the material for commercial purposes.
As of 2025 authors retain their copyright and assign to the journal the right of first publication of their work, which shall simultaneously be subject to the license https://creativecommons.org/licenses/by-nc-sa/4.0/deed.es that permits sharing, copying and redistribution of the material in any medium or format provided that initial publication in this journal is indicated. Adapt, remix, transform and build upon the material. If you remix, transform, or build from the material, you must distribute your contribution under the same license as the original and may not make use of the material for commercial purposes.
Under the following terms:
1. Attribution: you must give proper credit, provide a link to the license, and indicate whether changes have been made. You may do so in any reasonable manner, but not in such a way as to suggest that you or your use is endorsed by the licensor.
2. NonCommercial: you may not use the material for commercial purposes.
3. ShareAlike: if you remix, transform or build upon the material, you must distribute your contribution under the same license as the original.




PlumX Metrics