Experiencia del Cirujano como riesgo de infección de sitio quirúrgico
DOI:
https://doi.org/10.35954/SM2005.27.1.4Keywords:
Surgical Block; Surgery; Wound Infection; Infections; Operating Room.Abstract
Introduction: Despite technical advances, greater knowledge of the pathogenesis of wound infection and the use of prophylactic antibiotics, surgical site infection (SSI) continues to be an important morbimortality factor. It is estimated to account for 24% of hospital-acquired infections, ranking second only to urinary tract infections among nosocomial infections (1).
Among the risk factors that have been associated with surgical site infection, surgical technique is considered one of the factors that play a fundamental role in postoperative complications, including infection (1,2,3 ).
The main risk factors are linked to inadequate cleaning of the surgical site, hematoma formation and increased tissue exposure time (duration of surgical time). These factors should be improved as the surgeon's experience increases (4).
The purpose of this study is to determine the importance of the surgeon's experience as a risk factor in the development of surgical site infection in a specific intervention: cholecystectomy by laparotomy.
Methodology: This is a retrospective cohort study of patients who underwent cholecystectomy at the Central Hospital of the Armed Forces between 1999 and 2003.
A sample size was estimated with the epi info 6.0 statcal program.
The main independent variable of the study was the surgeon's experience, which was categorized into two groups, resident and surgeon, and the primary outcome was surgical site infection.
The distribution of patient characteristics between surgeons and residents was analyzed with chi-square.
Univariate and multivariate analysis was used to determine the association between the different variables and the outcome of interest.
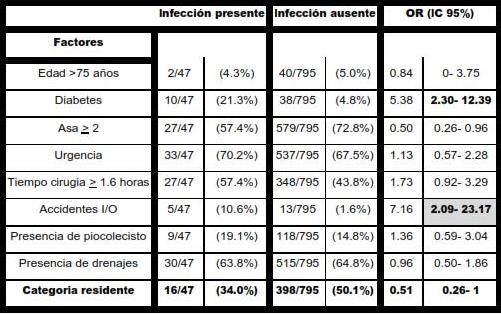
Results: A total of 842 cholecystectomized patients were followed and the presence of diabetes OR 5.3 (2.26-12.5), the severity score >2 loop OR 2.41 (1.22-4.75) and the presence of intraoperative accidents OR 3.60 (1.08-11.9) were undoubted independent predictors.
Surgery performed by residents showed a borderline interval OR 1.91 (1.0-3.62).
Conclusion: Surgeon experience shows an incidence in this work and for this population as an independent predictor of surgical site infection.
Downloads
References
(1) GLEN MAYHALL, Hospital Epidemiology and Infection Control. WILLIAM WILKINS, Baltimore 1996, Second edition 1999.
(2) RICHARD P. WENZEL, Prevention and Control of Nosocomial Infections. WILLIAM WILKINS, Baltimore Second Edition 1993, Third Edition 1997.
(3) Center for Disease Control and Prevention. Guidelines for Prevention of Surgical Site Infection, 1999.
(4) CRUSE PJ, FOORD R. Epidemiología de las infecciones de heridas. Estudio durante 10 años de 62939 heridas. Clin. Quir. N.A. 1:25, 1980.
(5) Enciclopedia Medico Quirúrgica. Francia 2000.
(6) Text book of Surgery . U.S.A 2000.
(7) SOSA, COL. The importance of surgeon experience for clinical and economics outcomes from thyroidectomy. Ann Surg. Volume 228(3). September 1998. 320-330.
(8) ROTH, COL. Does the success of ureterointestinal implantation in orthotopic bladder substitution depend more on surgeon level of experience or choice of technique. J. Urol, Voluime 157(1). January 1997.56-60.
(9) WITT, COL. The effect of surgeon experience on velopharyngeal functional outcome following palatoplasty: Is there a learning curve? Plast Reconstr Surg 1998; 102(5):1375-1384.
Published
How to Cite
Issue
Section
License
Until 2024 we use the Creative Commons Attribution/NonCommercial Attribution 4.0 International License https://creativecommons.org/licenses/by-nc/4.0/deed.es. Which states that: you are free to share, copy and redistribute the material in any medium or format, as well as to adapt, remix, transform and build upon the material. Under the following terms:
Attribution: you must give proper credit , provide a link to the license, and indicate if changes have been made . You may do so in any reasonable manner, but not in such a way as to suggest that you or your use is endorsed by the licensor.
NonCommercial: you may not use the material for commercial purposes.
As of 2025 authors retain their copyright and assign to the journal the right of first publication of their work, which shall simultaneously be subject to the license https://creativecommons.org/licenses/by-nc-sa/4.0/deed.es that permits sharing, copying and redistribution of the material in any medium or format provided that initial publication in this journal is indicated. Adapt, remix, transform and build upon the material. If you remix, transform, or build from the material, you must distribute your contribution under the same license as the original and may not make use of the material for commercial purposes.
Under the following terms:
1. Attribution: you must give proper credit, provide a link to the license, and indicate whether changes have been made. You may do so in any reasonable manner, but not in such a way as to suggest that you or your use is endorsed by the licensor.
2. NonCommercial: you may not use the material for commercial purposes.
3. ShareAlike: if you remix, transform or build upon the material, you must distribute your contribution under the same license as the original.




PlumX Metrics